Face2Face Health: Face2Face Health
by Ami Shah
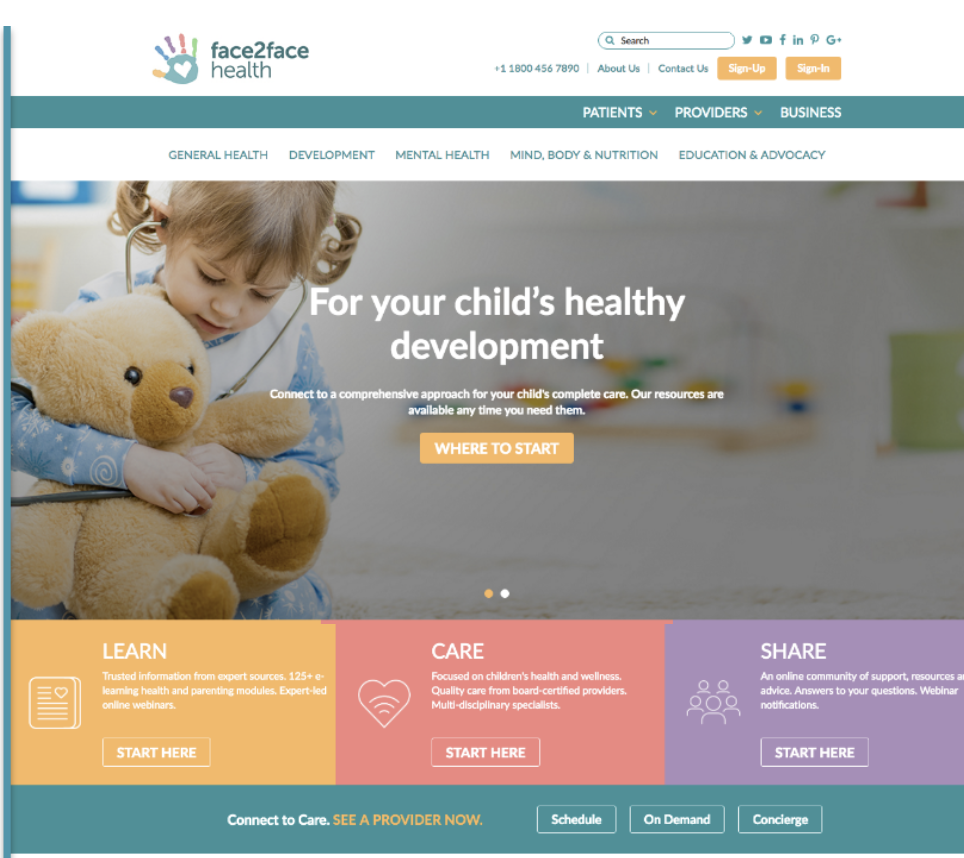
Face2Face Health is a transformative digital platform that provides parents with a single integrated, end-to-end resource to help optimize healthcare for their kids.
New York, NY United States Equity Raise WarOnCOVID challenge
About our project
The problem we solve: Surveys reveal that 88% of US adults are health illiterate to some degree, deleteriously impacting their kids’ well-being - ultimately affecting caregivers’ work performance and producing negative results for the economy. Consider: • Of the 90 million kids in the US, only 30% are screened for developmental issues • Delays in diagnosis cost corporate America $150 billion annually • Absenteeism costs corporate America $78 billion annually The core issue is a lack of comprehensive, coordinated, connected care - validated via 500+ multi-specialty providers and 1,000+ parents. 80% of US Internet users (93M Americans) have searched for health-related topics online, only to be met with a mish-mash of results from different sources - often conflicting – often unreliable. Despite healthcare tech advances, the disconnect persists. Effectively providing telemedicine for urgent care (addressing the symptom), fails to address the underlying cause with true end-to-end service.
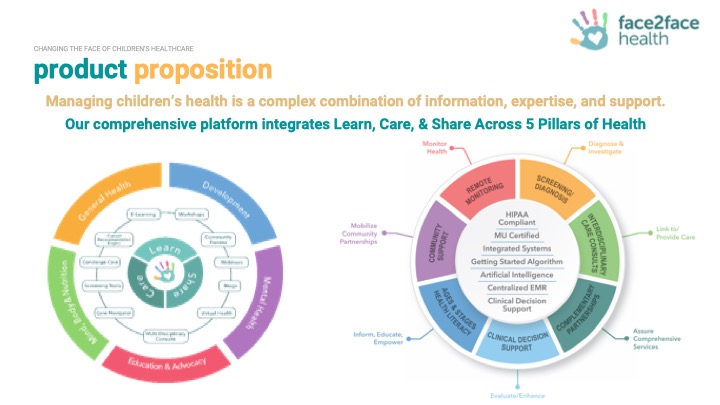
About our solution: We are a transformative digital health platform, providing parents with a single, end-to-end solution to help optimize healthcare for their kids. Our solution uniquely integrates health literacy e-learning courses; telemedicine access to multidisciplinary healthcare professionals, educators & advocates; expert-led webinars; & web-forum communities for sharing knowledge & support across 5 pillars of care: General Health, Emotional Health, Development, Mind/Body/Nutrition, and Education/Advocacy.
Progress to date:
Commercial and Technical Milestones
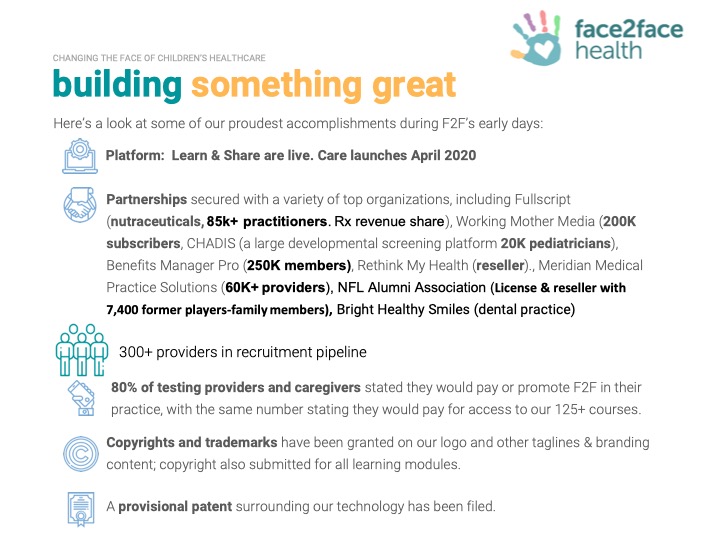
Learn and Share: live with Working Mother Media (200K subscribers), Living 2.0 (1,500 associations), Meridian Medical Practice Solutions, (80K providers), Bright Health Smiles dental (patient promotions), NFL Alumni Association (member promotions), Chadis, credible screening platform (20K pediatricians), Fullscript, Nutraceuticals, Mint Benefits (lead generation), Rethink My Therapy (reseller). United Nations (authorized to do business). Ask the Expert & CARE launch April, 2020. 300+ providers ready for CARE, positioned to scale quickly.
About Our Team

Creator: Ami Shah
Location: New York
Education: Wright State University School of Medicine
Bio: Ami Anand Shah, MD FACP, FAARM is an entrepreneur, pharmaceutical industry executive, active part- time integrative medicine practitioner, philanthropist and leader in several local, state and national medical non-profit organizational communities. She has over 15 years of both clinical practice and global versatile pharmaceutical industry executive experience with demonstrated leadership, people management and global expertise in the arenas of pharmacovigilance and risk management, clinical development, strategic business development/due diligence, global labeling, OTC/nutritionals formulation, clinical trial development and medical marketing from small sized to big sized pharmaceutical companies. She is a Board Certified Internal Medicine physician and fellow of the American College of Physicians, Board Certified in Integrative Medicine and is also fellowship trained in Anti-aging, Regenerative and Functional Medicine as well as Aesthetics and currently practices part-time Integrative, Personalized Medicine which focuses on integrative evidence based, peer reviewed holistic health, e consulting, physician health coaching, and telemedicine services for over 15 years. Dr. Shah has held several leadership positions at the local, state and national levels (see Affliations section) To date, she has mentored several next generational leaders, performs various free health care services in clinics or lectures in the community and has travelled to over 20 countries on medical missions. Dr. Shah is also a member of countless other non-profit organizations too numerous to name but have in common a focus on children and women’s global health and education issues. She has been the recipient of the prestigious top 50 Outstanding Asian Americans in business 2012 and is also featured as one of the top 101 Indian American Emerging and Global Leaders by Roshni Media published in 2015.
Hospital Affiliation: ACP Fellow, NY Country Medical Society, SAHI, AAPI, Clinical Associate Prof, Wright State University
Title: Founder & CEO
Advanced Degree(s): MD FACP, FAARM
About Team Members
Dale McManiis
Head of Education and Advocacy, BS, MEd, PHD
Biography: Lilla Dale McManis is President and CEO of Parent in the Know and Early Childhood Research
Solutions, launched to focus on assessment of the parental role and child functioning, and a consultant for numerous start-ups to improve and position products and services. She holds a PhD in educational psychology with a concentration in learning and cognition, a master’s in special education, and a bachelor’s in child development. She has taught special needs K-12 students in the public-school setting, served as Academic Coordinator and instructor for court-ordered teens in a non-traditional educational setting and as an instructor of prospective teachers at the University of Florida. She has held senior research positions at the Massachusetts Department of Education as lead evaluator for the state’s school health programs and the Massachusetts Department of Public Health in the Division of Maternal and Child Health as Project Manager for the state’s school and adolescent programs and Co-Director of the Office of Statistics and Evaluation. She was on the faculty at the University of Texas-Houston in the School of Public Health and then the Medical School-Developmental Pediatrics in the Children’s Learning Institute and the State Center for Early Childhood Development as part of multi-disciplinary teams on CDC, USDOE, and NIMH research grants. She is the former Research Director for Hatch Early Learning, a leading technology content development company, where she was on the product development team and conducted product efficacy studies. She is a founding member of the Early Childhood Technology Collaborative, has served as research consultant on a number of large projects, presented frequently at national conferences, & has published a number of academic
papers. She has been inducted into several honor societies: Golden Key, Phi Kappa Phi,
& Phi Lambda Theta graduated summa cum laude, on the National Dean’s List, and received the Gamma Sigma Delta Outstanding Senior Award.
Title: Head of Education and Advocacy
Advanced Degree(s): BS, MEd, PHD
LinkedIn:
https://www.linkedin.com/in/dalemcmanisecars/
Jennifer Kirschenbaum
General Counsel, BA, JD
Biography: Jennifer Kirschenbaum is a managing partner of Kirschenbaum & Kirschenbaum, P.C.'s healthcare department. She devotes her practice towards assisting practitioners in all aspects of private practice, Office-Based Surgery practice, Article 28 facility formation and operation, Independent Practice Association formation and operation and hospital based practice and hospital relationships/arrangements. Jennifer began her career focusing on third party payor and government payor audit defense, OPMC and OPD licensure matters and general practice matters, including license agreements, during her time as an associate at Abrams Fensterman, et al. Her practice expanded when she joined Rivkin Radler LLP, where she focused on regulatory compliance and transactional matters. After bringing healthcare to Kirschenbaum and Kirschenbaum, P.C. in 2008, Jennifer has grown the firm's healthcare department to representing over 800 practices, Article 28 facilities, IPAs and small to mega-group private practices. K&K's healthcare department represents MDs, DOs, DPMs, DDS, DMDs, DCs, PTs as well as other practitioners. Jennifer operates the healthcare department in conjunction with the other practice areas of law at the firm. When necessary our litigation, real estate, trust and estates or bankruptcy attorneys are available to assist in matters related to healthcare, issues involving practice break-ups, trademark infringement, breach of contract, etc. Practitioners contact Jennifer at all stages of practice, from their first employment agreement review and negotiation, their first lease, first partnership agreement, first patient issue, first lawsuit, first HIPAA complaint, first hospital contract, collection issues, audit through partnership structuring, mergers and acquisitions, practice sale, hospital employment or closure and everything in between. We are here to assist in any and all issues that arise that cannot be easily addressed internally or require third party consultation.
Title: General Counsel
Advanced Degree(s): BA, JD
LinkedIn:
https://www.linkedin.com/in/jennifer-kirschenbaum-1a169a17/
Dominic Ambrosio
Chief Operating Officer, MA
Biography: Mr. Dominic Ambrosio is an accomplished senior media and business development executive who stands at the forefront of the media industry, utilizing cutting edge technology to connect consumers with a wide array of content. Throughout his distinguished career, Mr. Ambroiso gained extensive production experience in film, television, digital media, e-commerce, web, mobile, wellness, nutrition, video retailing, product development, and broadcast operations. He specializes in developing diverse media operations in competitive markets for companies of all sizes from Fortune 500 to mid-sized and start-ups.
Mr. Ambroiso’s most recent achievement was launching two digital health startups between 2013 and 2017—Healthy Food Now, an online healthy food ordering delivery service and Rejuvenan Global Health, a visionary health integration platform that delivers evidence-based science of wellness to empower members to take control of their health and healthcare. As a senior, founding executive for RGH, Mr. Ambroiso was integral in all aspects of the image, content creation, and business development of this emerging sector.
Prior to that, Mr. Ambroiso honed his craft for three decades and held multiple leadership positions within the media and entertainment industry as follow:
Showtime Entertainment, Superviser/Producer
The Entertainment Channel (A&E), Production Manager
Unitel Video, Editor.
The Home Shopping Network, Senior Vice President of Network Operations
Speer Productions, Vice President Production
Home Box Office, Vice President of Studio Operations
During this time, Mr. Ambrosio served as an Adjunct Professor, at Kean University, Montclair State University, and the College of New Jersey.
Mr. Ambrosio holds a Master of Arts in Communications Arts from New York Institute of Technology and a Bachelor of Arts in Communications, specializing in Film/Television, from Seton Hall University.
Title: Chief Operating Officer
Advanced Degree(s): MA
LinkedIn:
www.linkedin.com/in/dominicambrosio1/
Monica Hein
Chief Digital Officer, BA
Biography: Ms. Monica Hein is a results-oriented global executive with general management, technology, sales, marketing, entrepreneurial, and business skills. She has extensive experience leading startup organizations as well as leading teams of up to 4,000 professionals. She is a decisive and strategic leader who is passionate about innovation and leading organizations to success. She has gained brand recognition for her ability to drive successful business outcomes with finesse and agility. She is adept at scaling new businesses and turnarounds to multi-billion $ sizes.
Ms. Hein has a proven track record building and operating successful businesses in the hi-tech industry. With 25 years of experience, she has gained unique perspectives across startup and Fortune 500 companies, having held key leadership roles within startup companies, juxtaposed with having launched new ventures within mature companies. She has built new business segments from the ground up and grown them into global organizations with significant revenue streams and YoY growth.
Ms. Hein is an accomplished speaker and has been a keynote presenter at various events. She has been named Woman of Influence by the Silicon Valley Business Journal. She was also named Best CIO Rising Star honoree by the Silicon Valley Business Journal. She has a keen interest in entrepreneurship and startups, and is an investor, board advisor, and mentor in the tech industry.
She is a Charter Member with TiE (The Indus Entrepreneurs).
Title: Chief Digital Officer
Advanced Degree(s): BA
LinkedIn:
www.linkedin.com/in/monicahein/
Zarme Shahnawaz
Medical Director, MBBS, BSc(med), FRACGP, CHC, MEHP Fellow
Biography: Dr. Zarme Shahnawaz is a primary care physician and integrative health coach, with a passion for holistic and preventative care, patient advocacy and medical education. She serves as the Medical Director and medical Advisory Board Member at Face2Face Health. She is lso engaged in private integrative health coaching as well as family practice. Prior experience includes medical entrepreneurship as cofounder of beSurgeryWise LLC, a holistic pre-habilitation service designed for patients undergoing major surgery. and Co-founder of Cue-rated LLC, a platform for the promotion of South Asian arts, culture and entrepreneurship.
Title: Medical Director
Advanced Degree(s): MBBS, BSc(med), FRACGP, CHC, MEHP Fellow
LinkedIn:
https://www.linkedin.com/in/zarme-shahnawaz-b7b583155/
Bryan Kawira
CTO, MBA
Biography: Tech development, big data analytics and tech lead health innovations experience.
Title: CTO
Advanced Degree(s): MBA
LinkedIn:
https://www.linkedin.com/in/bryan-kawira/
About Our Company

Face2Face Health
Location: Address: 236 East 82nd Street
Unit 1F
New York, NY 10028
US
Founded: 2014
Blog: https://blog.face2facehealth.com
Facebook: https://www.facebook.com/f2fhealth/
Other link: https://www.instagram.com/f2fhealth/
Product Stage: In the Market
Employees: 5-10
Challenge Mission
COVID Problem We Address
Face2Face Health helps with the COVID 19-related problems:
- Lack of safe, convenient access to COVID 19 prescreening
- Lack of safe, convenient access to comprehensive care
- Inability for many clients to see their providers in-office
- Lack of access to expert advice
- Emotional issues such as anxiety, depression, or grief
- Difficulty managing children at home, particularly when routines are disrupted
- Concerns about children’s education while schools are closed
- The need for a supportive community
- The need for expert, vetted education and information during a time rampant with misinformation
- Providers’ inability to see patients at their office
- Overwhelmed hospitals and clinics
Our COVID Solution
The F2F innovation will address the COVID-related problems in the following ways:
For parents and children who cannot conveniently nor safely see a provider, they can access, 24/7, from home consultations with experts on a variant of topics related to our 5 pillars of health: General Health, Emotional Health, Development, Mind, Body, Nutrition, and Education and Advocacy. The platform allows them to:
- Consult a provider for COVID 19 Prescreening
- Ask and Expert for advice
- Consult a Multi-Disciplinary provider team
For providers who currently cannot see clients in their office, they now how a way to continue their practice.
We have developed Targeted COVID-Relevant Courses that include Apps, Toys, Games, Books, Organizations, that will help sheltering-at-home parents and children with issues such as:
- Parenting skills
- Learning at home
- Caring for children with special needs
- Dealing with disrupted routines
- Managing stress and anxiety during uncertain times
We are producing a series of Expert-Webinars that will address COVID 19-related topics and are offering these webinars (live and recorded) free of charge.
Our online community forums offer users tips, resources and support.
Innovation Details
Intellectual Property Summary
Patent pending on machine learning to guide clinical decisions.
Clinical Information
A July 2015 American Academy of Pediatricians Technical Report cited the following ways that telemedicine is contributing to improving the practice of pediatrics and to the health of children:
Telemedicine is a technological tool that is improving the health of children around the world. … telemedicine’s current use bears testimony to its effectiveness and potential.
Children younger than 15 years old in the United States make an estimated 71 million office visits annually for acute problems, which are the leading cause of parents having to miss time from work. Clearly, the social and economic burden associated with caring for ill children is substantial. Opportunities exist to rethink how and when children receive medical care.
Pediatricians can use telemedicine for a broad range of applications. Telemedicine can be used for tele-education, teleconsultation, telepractice, and teleresearch.
Tele-education can connect academic medical center physicians with community physicians and offer current and cost-effective CME for local providers.
Tele-education can also provide credible, reliable information to patients and families.
Telepractice in the pediatric medical home eliminates access barriers, increases consumer satisfaction, preserves the integrity of the pediatric medical home, and prevents the fragmentation of care common with standalone direct-to-consumer telehealth care providers.55 Medical home–based telehealth visits can reduce emergency department visits for nonurgent care, thus preventing overcrowding and waste of health care dollars.
Teleconsultation overcomes the barriers of time and distance, allowing specialists, such as pediatric hospitalists, emergency medicine specialists, and critical care physicians, to bring their skills to the bedside of the child in need.
Teleresearch has become more sophisticated, progressing from user satisfaction and validation surveys to more complex outcome studies.
Pediatrics
July 2015, VOLUME 136 / ISSUE 1
From the American Academy of Pediatrics
Technical Report
Telemedicine: Pediatric Applications
Bryan L. Burke Jr, R. W. Hall, the SECTION ON TELEHEALTH CARE
http://pediatrics.aappublications.org/content/136/1/e293
A June 2015 American Academy of Pediatrics Policy Statement, “The Use of Telemedicine to Address Access and Physician Workforce Shortages,” cited several ways in which telemedicine “has the potential to transform the practice of pediatrics”. The Committee on Pediatric Workforce wrote:
As the use of telemedicine increases, it is likely to impact health care access, quality, and education and costs of care. Telemedicine technologies, applied to the medical home and its collaborating providers, have the potential to improve current models of care by increasing communication among clinicians, resulting in more efficient, higher quality, and less expensive care. Such a model can serve as a platform for providing more continuous care, linking primary and specialty care to support management of the needs of complex patients. In addition, telemedicine technologies can be used to efficiently provide pediatric physicians working in remote locations with ongoing medical education, increasing their ability to care for more complex patients in their community, reducing the burdens of travel on patients and families, and supporting the medical home.
Pediatrics
June 2015
From the American Academy of Pediatrics
Policy Statement
The Use of Telemedicine to Address Access and Physician Workforce Shortages
COMMITTEE ON PEDIATRIC WORKFORCE
http://pediatrics.aappublications.org/content/early/2015/06/23/peds.2015-1253
Telemed J E Health. 2017 Jul 21. doi: 10.1089/tmj.2017.0075. [Epub ahead of print]
Usability, Acceptability, and Impact of a Pediatric Teledermatology Mobile Health Application.
Fiks AG1,2,3, Fleisher L1,2,3, Berrigan L1, Sykes E1, Mayne SL1, Gruver R1, Halkyard K1, Jew OS1, FitzGerald P4, Winston F1,2,3,4, McMahon P1,2.
Author information
Abstract
OBJECTIVE:
Pediatric dermatology appointment wait times often exceed several months. We evaluated the usability, acceptability, and clinical impact of a store-and-forward teledermatology mobile application (app) linking families with pediatric dermatologists.
METHODS:
Parents of children age 6 weeks to 17 years or individuals 18-21 years old were invited (by e-mail or referral) to participate in this single group, prospective study. Within the app, users photographed the skin condition, answered questions, and submitted their case for review. One pediatric dermatologist viewed cases, diagnosed conditions, and provided instructions and prescriptions. User surveys immediately following app use and 1 week later, supplemented by electronic logs, assessed usability, acceptability, and impact.
RESULTS:
One hundred ninety-seven parents and one adolescent submitted cases within 39 days of invitation. App users were more likely to be white than those in the population invited (67% vs. 34%, p < 0.001) and their children were slightly younger (mean 7.3 vs. 9.0 years, p < 0.001). A majority, 83% found the app easy to use, 97% felt that submitting a case took "the right amount of time," 87% were satisfied, and 93% would use the app again. Prescription receipt was associated with increased app satisfaction (p = 0.008). The median user received a response in 2.8 h (interquartile range 1.1-6.4). Had the app been unavailable, 44% reported that they would have waited for primary care, 32% for a dermatology appointment, and 7% would have gone to an urgent care clinic.
CONCLUSIONS:
A mobile health app allowing families to directly consult a pediatric dermatologist was usable, acceptable, and expedited care.
KEYWORDS:
dermatology; m-health; pediatrics; teledermatology; telehealth; telemedicine
Pediatr Rheumatol Online J. 2017 Jul 11;15(1):55. doi: 10.1186/s12969-017-0184-y.
Telemedicine and other care models in pediatric rheumatology: an exploratory study of parents' perceptions of barriers to care and care preferences.
Bullock DR1, Vehe RK2, Zhang L3, Correll CK2.
Author information
Abstract
BACKGROUND:
The United States pediatric rheumatology workforce is committed to a mission of providing children access to pediatric rheumatology care. With a limited number and distribution of pediatric rheumatologists, telemedicine has been proposed as one way to meet this mission, yet the adoption of this modality has been slower than expected. The purpose of this study was to explore the parent perspective on barriers to accessing pediatric rheumatology care and to explore the acceptability of telemedicineand other alternative care models.
METHODS:
Over a period of six weeks, all new and return English-speaking parents/guardians of patients visiting a single center were offered an opportunity to complete a survey which assessed barriers to care and interest in alternative models of care. Responses were analyzed using descriptive statistics.
RESULTS:
Survey response rate was 72% (159/221). Twenty-eight percent (45/159) traveled more than three hours to the pediatric rheumatology clinic, and 43% (65/152) reported travel as inconvenient. An overwhelming majority of respondents (95%, 144/152) reported a preference for in-person visits over the option of telemedicine. This preference was similar regardless of whether respondents reported travel to the clinic as inconvenient vs convenient (inconvenient 92%, 60/65; convenient 97%, 84/87; p = 0.2881) and despite those reporting travel as inconvenient also reporting greater difficulty with several barriers to care. Those familiar with telemedicine were more likely to report a preference for telemedicine over in-person visits (27%, 3/11 vs 3%, 4/140; p = 0.0087). The option of an outreach clinic was acceptable to a majority (63%, 97/154); however, adult rheumatology and shared-care options were less acceptable (22%, 35/156 and 34%, 53/156 respectively).
CONCLUSION:
Among survey respondents, in-person visits were preferred over the option of telemedicine, even when travel was noted to be inconvenient. Telemedicine familiarity increased its acceptability. Outreach clinics were acceptable to a majority. Ultimately, the parent perspective can shape acceptable ways to address barriers and provide accessible care.
KEYWORDS:
Access; Barriers; Outreach; Pediatric rheumatology; Telemedicine
PMID: 28693580
PMCID:PMC5504634
DOI: 10.1186/s12969-017-0184-y
J Adolesc Young Adult Oncol. 2017 Jun 28. doi: 10.1089/jayao.2017.0013. [Epub ahead of print]
Shared Care of Childhood Cancer Survivors: A Telemedicine Feasibility Study.
Costello AG1, Nugent BD2,3, Conover N1,3, Moore A1, Dempsey K1, Tersak JM1,3.
Author information
Abstract
PURPOSE:
With an increasing number of childhood cancer survivors (CCSs), determining the best model of survivorship transition care is becoming a growing priority. Shared care between pediatric oncology and adult primary care is often necessary, making survivorship a time of transition, but effective standard models are lacking. We sought to provide a more integrated approach to transition using telemedicine.
METHODS:
Recruited primary care provider/CCS dyads were instructed to log-in to a password-protected virtual meeting room using telemedicine equipment at the time or a regularly scheduled office visit. Dyads were joined by a pediatric survivorship clinic team member who conducted the telemedicine portion of the transition visit, which consisted of the review of an individualized treatment summary and care plan. Postquestionnaires were developed to evaluate key points such as fund of knowledge, satisfaction with the visit, and effectiveness of this electronic tool.
RESULTS:
There were 19 transition visits conducted, 13 of which used the telemedicine equipment as planned. Those that did not use the equipment were primarily unable to due to technical difficulties. Postquestionnaires were overall positive, confirming increased knowledge, comfort and abilities, and patient satisfaction in survivorship care. Negative comments were primarily related to equipment difficulties.
CONCLUSIONS:
A gap still remains in helping CCSs transition from oncology to primary care and this pilot study offered insights into how we might better bridge that gap through the use of telemedicine. Further research is needed to refine the transition process for CCSs, including evaluation and testing models for standard of care.
KEYWORDS:
childhood cancer; late effects; primary care; survivorship; telemedicine; transition
PMID: 28657408
Mhealth. 2017 May 11;3:19. doi: 10.21037/mhealth.2017.04.03. eCollection 2017.
Understanding potential uptake of a proposed mHealth program to support caregiver home management of childhood illness in a resource-poor setting: a qualitative evaluation.
Calderón TA1, Martin H2, Volpicelli K3, Frasso R4, Díaz Arroyo EC5, Gozzer E5, Buttenheim AM6,7.
Author information
Abstract
BACKGROUND:
Extensive uptake of mobile phones offers an unprecedented opportunity to improve global healthcare delivery, especially among underserved populations. Mobile health (mHealth) has been increasingly recognized as a promising approach to addressing challenges in global maternal-child health and may play an important role in accelerating progress towards improved outcomes. However, more evidence guiding development of mHealth interventions is needed. The current study explores factors that may support or hinder adoption and use of a proposed mHealth intervention to improve caregiver home management of common childhood illnesses in order to shape program development.
METHODS:
Elicitation interviews were conducted with a convenience sample of 25 mothers recruited from a larger cluster-randomized survey sample in the Cono Norte region of Arequipa, Peru. Interview data were analyzed in Spanish to preserve important cultural nuances.
RESULTS:
Thematic analysis revealed potential facilitators of and barriers to uptake of the proposed mHealth program. Potential facilitators of caregiver participation include opportunity to engage in two-way communication with healthcare providers, development of instrumental and support knowledge to care for sick children, and healthcare challenges faced in a resource-poor community. Potential barriers include preference for in-person healthcare visits, program cost, text messaging abilities, and concern around program legitimacy.
CONCLUSIONS:
This study underscores the potential for mHealth to improve global healthcare delivery in the area of maternal-child health. It demonstrates that mHealth interventions can meet the needs of vulnerable populations by offering novel approaches to promoting evidence-based care. This in-depth understanding of factors that may influence participation and use of this proposed mHealth program will help shape development of the intervention in this community.
KEYWORDS:
Peru; Telemedicine; global health; qualitative research
PMID: 28607905
PMCID: PMC5460105
DOI:10.21037/mhealth.2017.04.03
Rural Remote Health. 2017 Apr-Jun;17(2):3965. doi: 10.22605/RRH3965. Epub 2017 May 31.
Feasibility of developing a pediatric telehealth network in Honduras with international consultation support.
Brooks M1, Holden KR2, Durón RM3, McElligott JT4, Summer A5.
Author information
Abstract
INTRODUCTION:
Honduras is the second poorest country in Central America, and roughly 50% of the population lives in rural areas. A telehealth network linking these areas to larger health centers may improve patient access to care, and physician access to educational opportunities. This pilot study assessed the feasibility of establishing a pediatric telehealth network between underserved clinics in Honduras and the Medical University of South Carolina (MUSC).
METHODS:
Two underserved Honduran clinics were identified and invited to participate in the telehealth network. Providers from these clinics connected remotely to educational conferences at MUSC, and received teleconsults from MUSC physicians and physicians from the other Honduran site. Honduran providers completed five-point Likert scale satisfaction surveys following participation in the conferences and teleconsults.
RESULTS:
Survey feedback was positive, with 100% of respondents stating they would utilize telemedicine in the future. Dissatisfaction was expressed subjectively in the survey comments with regards to poor Internet connectivity and unreliable electrical power.
CONCLUSIONS:
The establishment of a telehealth network between Honduras and MUSC is feasible, and rural providers were receptive to the clinical and educational opportunities this network provides. Future projects will expand telehealth capabilities to other Honduran sites and focus on intra-country collaboration to ensure sustainability.
KEYWORDS:
Education; Medical; Paediatrics; Postgraduate
PMID:28564548
DOI: 10.22605/RRH3965
Pediatrics. 2017 May;139(5). pii: e20170629. doi: 10.1542/peds.2017-0629.
Nonemergency Acute Care: When It's Not the Medical Home.
Conners GP, Kressly SJ, Perrin JM, Richerson JE, Sankrithi UM; COMMITTEE ON PRACTICE AND AMBULATORY MEDICINE; COMMITTEE ON PEDIATRIC EMERGENCY MEDICINE; SECTION ON TELEHEALTH CARE; SECTION ON EMERGENCY MEDICINE; SUBCOMMITTEE ON URGENT CARE; TASK FORCE ON PEDIATRIC PRACTICE CHANGE.
Collaborators (53)
Abstract
The American Academy of Pediatrics (AAP) affirms that the optimal location for children to receive care for acute, nonemergency health concerns is the medical home. The medical home is characterized by the AAP as a care model that "must be accessible, family centered, continuous, comprehensive, coordinated, compassionate, and culturally effective." However, some children and families use acute care services outside the medical home because there is a perceived or real benefit related to accessibility, convenience, or cost of care. Examples of such acute care entities include urgent care facilities, retail-based clinics, and commercial telemedicine services. Children deserve high-quality, appropriate, and safe acute care services wherever they access the health care system, with timely and complete communication with the medical home, to ensure coordinated and continuous care. Treatment of children under established, new, and evolving practice arrangements in acute care entities should adhere to the core principles of continuity of care and communication, best practices within a defined scope of services, pediatric-trained staff, safe transitions of care, and continuous improvement. In support of the medical home, the AAP urges stakeholders, including payers, to avoid any incentives (eg, reduced copays) that encourage visits to external entities for acute issues as a preference over the medical home.
Copyright © 2017 by the American Academy of Pediatrics.
PMID: 28557775
Acta Med Port. 2017 Apr 28;30(4):253-254. doi: 10.20344/amp.9034. Epub 2017 Apr 28.
[Coimbra Telemedicine Service Improves Access to Pediatric Cardiology in Cape Verde].
[Article in Portuguese]
Author information
KEYWORDS:
Cape Verde; Cardiology; Child; Heart Diseases; Pediatrics; Portugal; Telemedicine
PMID: 28555549
Paediatr Int Child Health. 2017 Aug;37(3):155-157. doi: 10.1080/20469047.2017.1315914. Epub 2017 May 12.
Telemedicine is helping the parents of children with neurodevelopmental disorders living in remote and deprived areas.
Stuckey R1, Domingues-Montanari S1,2.
Author information
Abstract
Telecommunication technologies are advancing rapidly with huge investment to improve infrastructure in rural areas. Telemedicine brings the benefits of telecommunication to healthcare, especially in resource-limited and remote communities. The recent literature on telemedicine in paediatrics will be reviewed, with particular focus on its application to help children with neurodevelopmental disorders and their families living in remote regions and/or low-income countries, and gaps identified for future research. Studies show that telemedicine can enable a family's access to appropriately qualified help that physically may only be available hundreds of miles away, helping to overcome geographic barriers. Telemedicine can also train parents and equip them with the knowledge and skills to better care for their children. Despite some technological barriers to implementation, telemedicine can help transform all stages of autism treatment. However, more studies are required in low- and middle-income countries to fully elucidate the benefits offered by telemedicine to autistic children and their families.
PMID: 28498062
DOI:10.1080/20469047.2017.1315914
JMIR Med Educ. 2017 May 10;3(1):e10. doi: 10.2196/mededu.5434.
Development and Assessment of an E-learning Course on Pediatric Cardiology Basics.
Oliveira AC1, Mattos S2, Coimbra M3.
Author information
Abstract
BACKGROUND:
Early detection of congenital heart disease is a worldwide problem. This is more critical in developing countries, where shortage of professional specialists and structural health care problems are a constant. E-learning has the potential to improve capacity, by overcoming distance barriers and by its ability to adapt to the reduced time of health professionals.
OBJECTIVE:
The study aimed to develop an e-learning pediatric cardiology basics course and evaluate its pedagogical impact and user satisfaction.
METHODS:
The sample consisted of 62 health professionals, including doctors, nurses, and medical students, from 20 hospitals linked via a telemedicine network in Northeast Brazil. The course was developed using Moodle (Modular Object Oriented Dynamic Learning Environment; Moodle Pty Ltd, Perth, Australia) and contents adapted from a book on this topic. Pedagogical impact evaluation used a pre and posttest approach. User satisfaction was evaluated using Wang's questionnaire.
RESULTS:
Pedagogical impact results revealed differences in knowledge assessment before and after the course (Z=-4.788; P<.001). Questionnaire results indicated high satisfaction values (Mean=87%; SD=12%; minimum=67%; maximum=100%). Course adherence was high (79%); however, the withdrawal exhibited a value of 39%, with the highest rate in the early chapters. Knowledge gain revealed significant differences according to the profession (X22=8.6; P=.01) and specialty (X22=8.4; P=.04). Time dedication to the course was significantly different between specialties (X22=8.2; P=.04).
CONCLUSIONS:
The main contributions of this study are the creation of an asynchronous e-learning course on Moodle and the evaluation of its impact, confirming that e-learning is a viable tool to improve training in neonatal congenital heart diseases.
KEYWORDS:
cardiology; congenital heart defects; continuing medical education; distance learning; pediatrics
PMID: 28490416
PMCID: PMC5443913
DOI: 10.2196/mededu.5434
Telemed J E Health. 2017 May 9. doi: 10.1089/tmj.2016.0251. [Epub ahead of print]
Use of Telehealth in Pediatric Palliative Care.
Winegard B1, Miller EG2, Slamon NB3.
Author information
Abstract
OBJECTIVES:
Pediatric subspecialty care, including multidisciplinary palliative care, tends to be located in urban academic centers or children's hospitals. Telehealth provides the opportunity to care for patients who would otherwise not be able to access services. We present cases wherein telehealth was used to provide counseling services to patients who would not have been able to receive this service.
METHODS:
We discuss cases of telehealth use for patient and family counseling in the setting of palliative care and bereavement follow-up. Patients who live a great distance from the hospital with limited access to services were followed by a hospital-based pediatric palliative care team. Patients and families gave feedback after use of telehealth for counseling services.
RESULTS:
Counseling through telehealth by our hospital-based palliative care social worker was successful for all parties involved: patient, family, and social worker.
CONCLUSIONS:
Telehealth helps relieve disparity in access to services and care, which is particularly problematic in pediatrics and mental health. For the patients in this case series, it was an effective modality to receive counseling services and meet needs that otherwise would not have been addressed.
KEYWORDS:
pediatrics; telecommunications; telehealth; telemedicine
PMID: 28486031
Acad Pediatr. 2017 Apr 18. pii: S1876-2859(17)30164-X. doi: 10.1016/j.acap.2017.04.008. [Epub ahead of print]
Development of School-Based Asthma Management Programs in Rochester, New York: Presented in Honor of Dr Robert Haggerty.
Halterman JS1, Tajon R2, Tremblay P2, Fagnano M2, Butz A3, Perry TT4, McConnochie KM2.
Author information
Abstract
In the spirit of Dr. Haggerty's teachings, we present an overview of our work to improve care for children with asthma in the context of 3 lessons learned: 1) the importance of providing integrated services across disciplinary boundaries for children with chronic illness, 2) the need to move from a care model focused only on the individual child to a model focused on the child, family, and community, and 3) the need to expand beyond the local community and take a broad perspective on improving health on a national level. The goal of our program is to develop sustainable models to overcome the multiple obstacles to effective preventive care for urban children with asthma. The primary intervention for our original School-Based Asthma Therapy program was directly observed administration of preventive asthma medications in school (with dose adjustments on the basis of National Heart, Lung, and Blood Institute guidelines). We found that children who received preventive medications in school through directly observed therapy had improved outcomes across multiple outcome measures. Our subsequent asthma programs have focused on dissemination and sustainability, with the incorporation of communication technology to enhance the system of care. We are currently testing the 'School-Based Telemedicine Enhanced Asthma Management' program, including 400 children with persistent asthma from the Rochester City School District. This program includes directly observed administration of preventive asthma medication at school, and school-based telemedicine to assure appropriate evaluation, preventive medication prescription, and follow-up care. It is designed to implement and sustain guideline-based asthma care through existing community infrastructure, and could serve as a model for the integration of services in rural as well as urban communities.
Copyright © 2017 Academic Pediatric Association. Published by Elsevier Inc. All rights reserved.
KEYWORDS:
asthma; chronic illness; prevention; telemedicine
PMID: 28434913
DOI:10.1016/j.acap.2017.04.008
Telemed J E Health. 2017 Apr 21. doi: 10.1089/tmj.2016.0236. [Epub ahead of print]
Family Perspectives on Telemedicine for Pediatric Subspecialty Care.
Ray KN1, Ashcraft LE2, Mehrotra A3, Miller E1, Kahn JM2,4.
Author information
Abstract
BACKGROUND:
Children often have difficulty accessing subspecialty care, and telemedicine may improve access to subspecialty care, but information is lacking on how best to implement telemedicine programs to maximize acceptance and, ultimately, maximize impact for patients and their families.
METHODS AND MATERIALS:
To understand how subspecialty telemedicine is perceived and to identify design elements with the potential to improve telemedicine uptake and impact, we conducted and analyzed semi-structured interviews with 21 informants, including parents and caregivers of children with subspecialty care needs and adolescent and young adult patients with subspecialty care needs.
RESULTS:
Although informants saw the potential value of using telemedicine to replace in-person subspecialty visits, they were more enthusiastic about using telemedicine to complement rather than replace in-person visits. For example, they described the potential to use telemedicine to facilitate previsit triage encounters to assess whether the patient was being scheduled with the correct subspecialist and with the appropriate level of urgency. They also felt that telemedicine would be useful for communication with subspecialists after scheduled in-person visits for follow-up questions, care coordination, and to discuss changes in health status. Informants felt that it was important for telemedicine programs to have transparent and reliable scheduling, same-day scheduling options, continuity of care with trusted providers, clear guidelines on when to use telemedicine, and preservation of parent choice regarding method of care delivery.
CONCLUSIONS:
Parents and patients articulated preferences regarding pediatric subspecialty telemedicine in this qualitative, hypothesis-generating study. Understanding and responding to patient and caregiver perceptions and preferences will be crucial to ensure that telemedicine drives true innovation in care delivery rather than simply recapitulating prior models of care.
KEYWORDS:
family centered; patient centered; pediatrics; policy; telehealth; telemedicine
PMID: 28430021
Telemed J E Health. 2017 Apr 20. doi: 10.1089/tmj.2016.0269. [Epub ahead of print]
Child and Adolescent Emergency and Urgent Mental Health Delivery Through Telepsychiatry: 12-Month Prospective Study.
Roberts N1, Hu T2, Axas N3, Repetti L3.
Author information
Abstract
BACKGROUND:
The significant gap between children and adolescents presenting for emergency mental healthcare and the shortage of child and adolescent psychiatrists constitutes a major barrier to timely access for psychiatric assessment for rural and remote areas. Unlike remote areas, urban emergency departments have in-house psychiatric consultation. Telepsychiatry may be a solution to ensure the same service for remote areas. However, there is a paucity of studies on the use of telepsychiatry for child and adolescent emergency consults. Thus, the aim of our study was to (1) assess patient satisfaction with telepsychiatry and (2) compare clinical characteristics and outcome of telepsychiatry with face-to-face emergency child and adolescent assessments.
METHODS:
This is a prospective study of telepsychiatry emergency assessments of children and adolescents referred by emergency physicians. The comparison group was age- and gender-matched patients seen for face-to-face urgent assessments. Data were gathered on demographic and clinical variables. Telepsychiatry satisfaction was assessed using a questionnaire. Descriptive statistics and chi-square tests were used to assess group differences for each variable. Logistic regression was used to assess impact of the variables on outcome after the consult. A p value <0.05 was used to determine statistical significance.
RESULTS:
Sixty (n = 60) assessments were conducted through telepsychiatry in 12 months. Among the telepsychiatry group, Aboriginal patients were over-represented (50% vs. 6.7%, p < 0.001), a higher proportion received a diagnosis of adjustment disorder (22% vs. 8.3%, p = 0.004) or no diagnosis (27% vs. 6.7%, p = 0.004) compared with controls. There was no statistically significant difference between groups on other clinical variables. Patients reported a high degree of satisfaction with telepsychiatry.
CONCLUSIONS:
Telepsychiatry is acceptable to patients and families for safe emergency assessment and follow-up, reducing unnecessary travel to urban centers. Longer time outcomes are needed to establish validity of telepsychiatry for emergency assessments.
KEYWORDS:
behavioral health; e-health; emergency medicine/teletrauma; pediatrics; telemedicine; telepsychiatry
PMID: 28426367
J Pediatr. 2017 Jun;185:181-186.e3. doi: 10.1016/j.jpeds.2017.02.054. Epub 2017 Mar 28.
Parent Participation in Pediatric Intensive Care Unit Rounds via Telemedicine: Feasibility and Impact.
Yager PH1, Clark M1, Cummings BM1, Noviski N1.
Author information
Abstract
OBJECTIVES:
To evaluate feasibility and impact of telemedicine for remote parent participation in pediatric intensive care unit (PICU) rounds when parents are unable to be present at their child's bedside.
STUDY DESIGN:
Parents of patients admitted to a 14-bed PICU were approached, and those unable to attend rounds were eligible subjects. Nurse and physician caregivers were also surveyed. Parents received an iPad (Apple Inc, Cupertino, California) with an application enabling audio-video connectivity with the care team. At a predetermined time for bedside rounds with the PICU team, parents entered a virtual meeting room to participate. Following each telemedicine encounter, participants (parent, physician, nurse) completed a brief survey rating satisfaction (0?=?not satisfied, 10?=?completely satisfied) and disruption (0?=?no disruption at all, 10?=?very disruptive).
RESULTS:
A total of 153 surveys were completed following 51 telemedicine encounters involving 13 patients. Parents of enrolled patients cited work demands (62%), care for other dependents (46%), and transportation difficulties (31%) as reasons for study participation. The median levels of satisfaction and disruption were 10 (range 5-10) and 0 (range 0-5), respectively. All parents reported that telemedicine encounters had a positive effect on their level of reassurance regarding their child's care and improved communication with the care team.
CONCLUSIONS:
This proof-of-concept study indicates that remote parent participation in PICU rounds is feasible, enhances parent-provider communication, and offers parents reassurance. Providers reported a high level of satisfaction with minimal disruption. Technological advancements to streamline teleconferencing workflow are needed to ensure program sustainability.
Copyright © 2017. Published by Elsevier Inc.
KEYWORDS:
communication; family-centered care; telemedicine
PMID:28363361
DOI:10.1016/j.jpeds.2017.02.054
J Clin Med. 2017 Mar 23;6(4). pii: E36. doi: 10.3390/jcm6040036.
Telemedicine Applications in Pediatric Retinal Disease.
Author information
Abstract
Teleophthalmology is a developing field that presents diverse opportunities. One of its most successful applications to date has been in pediatric retinal disease, particularly in screening for retinopathy of prematurity (ROP). Many studies have shown that using telemedicine for ROP screening allows a remote ophthalmologist to identify abnormal findings and implement early interventions. Here, we review the literature on uses of telemedicine in pediatric retinal disease and consider future applications.
KEYWORDS:
pediatrics; retina; retinopathy of prematurity; telemedicine screening; teleophthalmology
PMID:28333078
PMCID:PMC5406768
Pediatr Emerg Care. 2017 Mar 21. doi: 10.1097/PEC.0000000000001098. [Epub ahead of print]
Factors Associated With Discharge Home After Transfer to a Pediatric Emergency Department.
Peebles ER1, Miller MR, Lynch TP, Tijssen JA.
Author information
Abstract
OBJECTIVES:
The transfer of children from community emergency departments (EDs) to tertiary care pediatric EDs for investigations, interventions, or a second opinion is common. In order to improve health care system efficiency, we must have a better understanding of this population and identify areas for education and capacity building.
METHODS:
We conducted a retrospective chart review of all patients (aged 0-17 years) who were transferred from community ED to a pediatric ED from November 2013 to November 2014. The primary outcome was the frequency of referred patients who were discharged home from the pediatric ED.
RESULTS:
Two hundred four patients were transferred from community EDs in the study period. One hundred thirteen children (55.4%) were discharged home from the pediatric ED. Presence of inpatient pediatric services (P = 0.04) at the referral hospital and a respiratory diagnosis (P = 0.03) were independently associated with admission to the children's hospital. In addition, 74 patients (36.5%) had no critically abnormal vital signs at the referral hospital and did not require any special tests, interventions, consultations, or admission to the children's hospital. Younger age (P = 0.03), lack of inpatient pediatric services (P = 0.04), and a diagnosis change (P = 0.03) were independently associated with this outcome.
CONCLUSIONS:
More than half of patients transferred to the pediatric tertiary care ED did not require admission, and more than one third did not require special tests, interventions, consults, or admission. Many of these patients were likely transferred for a second opinion from a pediatric emergency medicine specialist. Education and real-time videoconferencing consultations using telemedicine may help to reduce the frequency of transfers for a second opinion and contribute to cost savings over the long term.
PMID: 28328691
DOI:10.1097/PEC.0000000000001098
JAMA Pediatr. 2017 May 1;171(5):461-469. doi: 10.1001/jamapediatrics.2017.0042.
Mobile Health Interventions for Improving Health Outcomes in Youth: A Meta-analysis.
Fedele DA1, Cushing CC2, Fritz A1, Amaro CM3, Ortega A1.
Author information
Abstract
IMPORTANCE:
Mobile health interventions are increasingly popular in pediatrics; however, it is unclear how effective these interventions are in changing health outcomes.
OBJECTIVE:
To determine the effectiveness of mobile health interventions for improving health outcomes in youth 18 years or younger.
DATA SOURCES:
Studies published through November 30, 2016, were collected through PubMed, Cumulative Index to Nursing and Allied Health Literature, Educational Resources Information Center, and PsychINFO. Backward and forward literature searches were conducted on articles meeting study inclusion criteria. Search terms included telemedicine, eHealth, mobile health, mHealth, app, and mobile application.
STUDY SELECTION:
Search results were limited to infants, children, adolescents, or young adults when possible. Studies were included if quantitative methods were used to evaluate an application of mobile intervention technology in a primary or secondary capacity to promote or modify health behavior in youth 18 years or younger. Studies were excluded if the article was an unpublished dissertation or thesis, the mean age of participants was older than 18 years, the study did not assess a health behavior and disease outcome, or the article did not include sufficient statistics. Inclusion and exclusion criteria were applied by 2 independent coders with 20% overlap. Of 9773 unique articles, 36 articles (containing 37 unique studies with a total of 29?822 participants) met the inclusion criteria.
DATA EXTRACTION AND SYNTHESIS:
Of 9773 unique articles, 36 articles (containing 37 unique studies) with a total of 29?822 participants met the inclusion criteria. Effect sizes were calculated from statistical tests that could be converted to standardized mean differences. All aggregate effect sizes and moderator variables were tested using random-effects models.
MAIN OUTCOMES AND MEASURES:
Change in health behavior or disease control.
RESULTS:
A total of 29?822 participants were included in the studies. In studies that reported sex, the total number of females was 11?226 (53.2%). Of those reporting age, the average was 11.35 years. The random effects aggregate effect size of mobile health interventions was significant (n = 37; Cohen d = 0.22; 95% CI, 0.14-0.29). The random effects model indicated that providing mobile health intervention to a caregiver increased the strength of the intervention effect. Studies that involved caregivers in the intervention produced effect sizes (n = 16; Cohen d = 0.28; 95% CI, 0.18-0.39) larger than those that did not include caregivers (n = 21; Cohen d = 0.13; 95% CI, 0.02-0.25). Other coded variables did not moderate study effect size.
CONCLUSIONS AND RELEVANCE:
Mobile health interventions appear to be a viable health behavior change intervention modality for youth. Given the ubiquity of mobile phones, mobile health interventions offer promise in improving public health.
PMID:28319239
DOI:10.1001/jamapediatrics.2017.0042
Nat Biotechnol. 2017 Apr;35(4):354-362. doi: 10.1038/nbt.3826. Epub 2017 Mar 13.
The Asthma Mobile Health Study, a large-scale clinical observational study using ResearchKit.
Chan YY1,2, Wang P1, Rogers L3, Tignor N1, Zweig M1, Hershman SG4, Genes N1,2, Scott ER1, Krock E4, Badgeley M1, Edgar R4, Violante S1, Wright R3,5,6, Powell CA3, Dudley JT1,7, Schadt EE1.
Author information
Abstract
The feasibility of using mobile health applications to conduct observational clinical studies requires rigorous validation. Here, we report initial findings from the Asthma Mobile Health Study, a research study, including recruitment, consent, and enrollment, conducted entirely remotely by smartphone. We achieved secure bidirectional data flow between investigators and 7,593 participants from across the United States, including many with severe asthma. Our platform enabled prospective collection of longitudinal, multidimensional data (e.g., surveys, devices, geolocation, and air quality) in a subset of users over the 6-month study period. Consistent trending and correlation of interrelated variables support the quality of data obtained via this method. We detected increased reporting of asthma symptoms in regions affected by heat, pollen, and wildfires. Potential challenges with this technology include selection bias, low retention rates, reporting bias, and data security. These issues require attention to realize the full potential of mobile platforms in research and patient care.
PMID:28288104
DOI:10.1038/nbt.3826
Pediatr Emerg Care. 2017 Feb 21. doi: 10.1097/PEC.0000000000001067. [Epub ahead of print]
A Qualitative Analysis of General Emergency Medicine Providers' Perceptions on Pediatric Emergency Telemedicine.
Kim JW1, Tiyyagura G, Langhan M.
Author information
Abstract
OBJECTIVE:
Most children in the United States are evaluated in general emergency departments (ED), which are staffed by practitioners who care for both adults and children and may have limited pediatric resources. The application of telemedicine in pediatrics is growing and has been shown to be effective in outpatient as well as critical care settings. Telemedicine has the potential to address disparities in access to pediatric emergency care. The objective of this study was to explore experiences of general ED providers with telemedicine and their perception about a potential video telemedicine program with pediatric ED providers.
METHODS:
Using qualitative methods, a purposeful sample of general ED providers (attending physicians and physician assistants) in 3 Connecticut hospitals participated in audio-recorded semistructured interviews. In line with grounded theory, 3 researchers independently coded transcripts, collectively refined codes, and created themes. Data collection and analysis continued in an iterative manner, past the point of theoretical saturation.
RESULTS:
Eighteen general ED providers were interviewed. Three themes were identified: (a) familiarity with use in adult stroke patients but limited practical experience with telemedicine; (b) potential uses for pediatric telemedicine (guiding pediatric differential diagnosis and management, visual diagnosis, alleviating provider fears, low-frequency high-stakes events, determining disposition, assessing level of illness, and access to subspecialty consultation); and (c) limitations of telemedicine (infrequent need and implementation barriers).
CONCLUSIONS:
General ED providers identified 7 specific potential uses of pediatric emergency video telemedicine. However, they also identified several limitations of telemedicine in caring for pediatric emergency patients. Further studies after implementation of telemedicine program and comparing provider perceptions with actual practice may be helpful. Furthermore, studies on telemedicine's effect on patient-related outcomes and studies on cost-effectiveness might be necessary before the widespread implementation of a telemedicine program.
PMID:28225376
DOI:10.1097/PEC.0000000000001067
Adv Chronic Kidney Dis. 2017 Jan;24(1):17-21. doi: 10.1053/j.ackd.2016.12.003.
Overview on the Challenges and Benefits of Using Telehealth Tools in a Pediatric Population.
Author information
Abstract
Telehealth in Pediatric Medicine presents many of the same benefits and challenges noted in adult-based medicine. In terms of health care delivery, the promise of improving access and reducing costs using telehealth in Pediatrics, particularly chronic care, is high. The ability to address clinician shortages and provide remote guidance for chronic care pathways from pediatric subspecialists to rural-based referring physicians is a developing model that represents a s
Regulatory Status
Not Applicable
How we will use the funds raised
This capital will allow us to deepen market penetration (especially through increased provider recruitment) while also stabilizing our platform and expanding course & content offerings. It will bridge us seamlessly into our Series A, valued at an estimated $5 million.
Specific capital allocation is as follows:
-
$600,000 for marketing
-
$500,000 for key hires
-
$300,000 for product development
-
$300,000 for content development
-
$300,000 for provider recruitment
Thank You
Face2Face Health originated from the Founder & CEO’s experience with her challenged twins. As a physician who personally experienced the pain and frustration of finding help, she decided to help other parents navigate the obstacles of a complex, confusing and often inaccessible medical system. 1/5 kids have challenges and are not meeting their full potential due to the current inadequacies of our medical system. Children lose and parents suffer. Face2Face Health provides parents and caregivers 24/7 access to experts consults with physicians, educators, coaches and advocates via online on-demand or scheduled visits, by phone or in their home. Our integrated approach to children’s health and wellness, parental education and online supportive communities is accessible in one convenient location dedicated to children’s health and wellness. Join us in our effort to revolutionize children’s healthcare.
Investor Info
Market Size
The average cost of an in-person healthcare visit is $176 - as opposed to just $40-50 for telemedicine. Here are a few other facts that further emphasize the outstanding market opportunity we have with F2F:
- $38B global telemedicine market in 2019 (projected to reach $130.5B by 2025)
- $190B global e-learning market in 2018 (projected to reach $300B by 2025)
- 80% of US Internet users have searched for health-related topics online
- The top 20 conditions F2F addresses cost our healthcare system $400B annually
- 15-20+ acquisitions occur in our industry annually (led by Teladoc & American Well)
Our primary target segment within this market is parents of children aged 18 or younger for the B2B2C and B2B sectors. These individuals are aware of the common conditions their kids face, but are struggling to obtain an in-depth understanding. The kids may also be newly diagnosed or need assistance with diagnosis, management or treatment of one of the conditions.
Secondarily, we will target HR & Employee Benefits departments of companies and other third-party associates for the B2B sector. These businesses generally suffer from a lack of employee productivity due to child illness & challenges and are actively seeking a better solution.
Projected 3 Year Growth
Financial Results and Projections (dollars in millions)
|
Fiscal Year |
2020 |
2021 |
2022 |
2023 |
2024 |
|
Revenue |
48,436 |
1,935,428 |
20,212,824 |
46,674,481 |
93,241,034 |
|
Gross Profit |
$23,413 |
$1,189,914 |
$12,193,319 |
$30,636,906 |
$62,042,606 |
Revenue Model
The all-encompassing nature of our platform places a wide variety of revenue opportunities at our disposal in ONE place. F2F is the very first solution of its kind to deliver healthcare providers with multiple revenue streams (including a referral program) aggregated into a single platform.
Our model is designed to capitalize through both target markets: 80% are focused on B2B & B2B2C, and 20% lean B2C.
Parent/Caregiver users can access Learn and Share for $79.95 annually, or $9.95/monthly. Our other revenue streams (across both target markets) are as follows:
- B2B2C licensing via per-member revenue share
- Affinity partnerships (% of sale)
- Web affiliates (% of sale)
- Per-member B2B licensing
- Telehealth consultation fees
- Custom webinar fees
- Diagnostic screening & assessments (% of sale)
- Content licensing fees
Price points for these streams are in line with subscription-level models used in similar services.
Competitors
The following 3 rivals pose the most significant direct threat to market share acquisition:
Maven Clinic | Multifaceted solution designed for women, providing a more direct outlet to child healthcare. Are well-funded and boast a simple, easy-to-navigate interface - but they fail to offer real education and don’t cover other health aspects (like mind-body).
Wildflower Health | Tech-centric platform that’s effective in giving parents the ability to track healthcare & well-being of both kids and aging parents. Being Alexa-enabled is an advantage, but they don’t have real education offerings and also cover limited topics.
Teladoc | Top telemedicine player with strong market share & a vast provider network, leaning on mobile videoconferencing technology. But despite their proven and efficient process, their traditional approach can be complex and the community aspect is lacking.
F2F’s “whole-istic” end-to-end approach - specifically, offering education, communities, and care in one place - is the primary differentiating factor we hold over these solutions.
The manner in which we empower the use to better care for their children is another big advantage - as F2F encourages addressing the underlying issue, not just symptoms.
Traction
- Partnerships secured with a variety of top organizations, including:
- Working Mother Media, 1.6M unique visitors; 100K digital subscribers; 100K print subscribers; 250 partner corporations
- CHADIS, a large developmental screening platform
- A voluntary benefits deal, Benefits Manager Pro, Living 2.0 (1,500 associations), and several others in the pipeline
- Fullscript, a leading virtual nutraceutical dispensary
- Meridian Medical Practice Solutions, promotions to 80K providers
- Bright Health Smiles dental practice
- Mint Benefits
- NFL Alumni
- ReThink My Therapy
- Deals in play:
- NYU College of Dentistry
- Asian American Business Development Center
- YMCA
- MommaWork leading provider of Corporate Lactation Support Services and New Parent Transition Coaching
- Web Exercises - clinical education, efficient and evidence-based exercise programming. Integration initiated
- United Nations - CEO is authorized to do business at the UN. Potential relationships with NGO's that support health and wellness.
Due Diligence Docs
Please note that access to the company's confidential materials is limited. Click this button to request access from the Company and its representatives.
Updates
No updates found .
Supporters
-

06/08/2020 - Liked the project. Instant Feedback
Instant Feedback
Help us find best new ideas to fund by telling us what you think. Your feedback goes straight to the team behind this project in private, so tell them what you really think.
34Medstartr
Index Score34
Interest
Score0
Adoption
Score4
Likes0
Partners0
Pilots0
Follows-
This campaign has ended but you can still get involved.See options below.
$ 2,000,000 goal
Instant Feedback
Help us find best new ideas to fund by telling us what you think. Your feedback goes straight to the team behind this project in private, so tell them what you really think.